Introduction of Ca. Prostate
Prostate cancer is the most common cancer in American men, with roughly 185,000 men diagnosed in 1998 and claiming 39,000 lives from it. Risk of developing this cancer increases with age and it is more common in men over ages 60-65. It is significantly more common in African-American men. Lifetime risk of developing this cancer is about 16-20% (1in 5 to 6).
It is estimated that 40% of men over age of 50 have microscopic areas of cancer in their prostate gland. However, only 8% of men will develop clinically significant disease and only 3% will die of this disease. Prostate cancer grows very slowly in older men and does not contribute to the cause of death in majority of cases.
Cause:
The cause of this cancer is unknown. However, certain factors increase the risk of developing prostate cancer:
- Increasing age
- African-American men
- Family history of prostate cancer
- High dietary fat
- Vasectomy
- Genetic factors
- Socioeconomic Status
- Cigarette smoking
- Occupational exposure to Cadmium Heavy metal
- Sexual activity and sexually transmitted illnesses
Patients do not have any signs at very early stages. As the disease progresses, patients may notice any of the following:
- Difficulty in urinating
- Burning while passing urine
- Increased frequency of urination
- Difficulty in starting the urine stream
- Blood in urine
- Pain while urinating
- Bone pain
- Swelling of legs
A cure of this cancer is possible when it is diagnosed at very early stages. Screening tests are performed on healthy individuals to detect cancers at very early stages, even before the cancer causes any signs.
PSA (prostate specific antigen) is a simple blood test. An elevated PSA blood level would hint at the possibility of prostate cancer and would be a strong indication to do a complete workup.
Digital rectal examination is very simple to perform and can detect lesions in rectum and prostate. This should be part of a routine physical exam for adults.
Establishing the diagnosis is achieved by taking a biopsy from the prostate tissue. This is done by Fine Needle Aspiration (FNA) of a trochar biopsy under ultrasound guidance. The biopsy sample is then sent to the pathologist for further study. Prostate cancer can be rendered a score based on the microscopic findings. This scoring system will determine the degree of aggressiveness of the cancer. Gleason Score is from two to ten, two being the least aggressive and ten the most aggressive kind of cancer.
Staging:
The next step after establishing the diagnosis is staging which is done by CT scan or MRI of pelvis and abdomen and bone scan.
Patterns of spread:
The disease can spread from prostate to the surrounding tissues, as well as to the pelvic lymph nodes, abdominal nodes, bone and lungs. This process may take years to decades, especially in the elderly. Most patients do not suffer from any major complications of this illness.
Treatment
To read more about it, click here.
Treatment
To read more about it, click here.
Special Situations
Patients with advanced prostate cancer may develop any of the following complications:
- Spinal cord compression
- Bone metastasis
- Para neoplastic syndromes
- High calcium level
- Pain
- High uric acid
- Pleural effusion
- Swelling of the legs
Survival of patients with advanced prostate cancer, in whom cure is not possible, could vary from months to years, depending on the extent of the cancer, the overall condition of the patient (as well as his response to treatment) and the duration of the response.
Family Member issues
First degree relatives of all patients with this cancer should be monitored carefully. This cancer has a tendency to run in families and be associated with genetic abnormalities, for which they can be tested for. Family members should consider genetic counseling to determine their risk and possible work up for early detection of the cancer.
Follow-up
After completion of treatment, in any combination that might have taken place, patients need to remain under surveillance for the possibility of recurrence of cancer. Follow-up shall be scheduled on a regular basis -- initially every one to three months for many years. The frequency of follow-up will depend on the condition of the patient and his disease. In each follow-up visit, the patient is examined and normally a PSA, and at times a CT scan of chest and abdomen and a bone scan is obtained
Treatment of the recurring disease will depend on the stage and extent of the recurring disease. Most patients are then treated with hormonal therapy, with the same agents as mentioned above. Radiation therapy may be helpful in managing painful or symptomatic areas in which the cancer has spread. If patients experience pain, various pain medications may be used to alleviate the pain. For patients with advanced disease, where most treatments have failed, one might consider assistance from hospice.
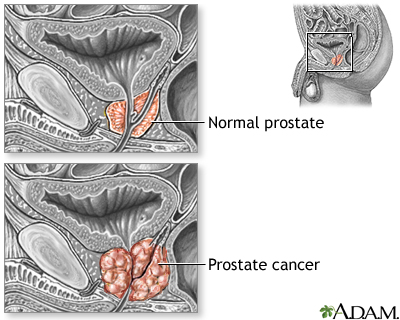


PROSTATE CANCER
PROSTATE CANCER
PROSTATE CANCER
PROSTATE CANCER